

Human Factors-Based Staff Decompression Zones in Regulated-Care Settings
A cost-effective, scalable model for staff recovery space design in long-term care facilities
The Problem
Long-term care facilities were among the hardest hit during the Covid-19 pandemic.Infection rates were stubbornly high and control efforts seemed to make minimal impact.
This work was done at the Design Institute for Health as part of an ongoing study sponsored by Austin Public Health.
I led concept development, design of the space and implementation.
Main factors affecting the system
Cross Section of Risk Factors - close living quarters, shared staff and services, and high medical frailty of patients.
Rapid Growth - In 30 years, the population in Texas over the age of 65 will triple. Those over 85 will quadruple by 2050.
Highly Regulated - The Nursing Home Reform Act of 1987 as well as thousands more federal, state and local level codes.

Areas for intervention
Infection control protocols
Actions and behaviors of staff
Design and management of facilities
Initial Pilot - infection control protocols
Following in-field primary research studies, an initial infection control pilot was launched - centering on a three-part entry protocol: stop, hand sanitize, replace gloves and mask. Visual cues at each patient room door reinforced the steps. The pilot produced no measurable reduction in COVID infection rates.
Researcher observations revealed that staff were routinely bypassing the protocol entirely. Post-pilot interviews surfaced the root cause: despite training, staff harbored deep frustration toward their work environment. They felt overworked, underpaid, and invisible to leadership — and that dissatisfaction translated directly into non-compliance.
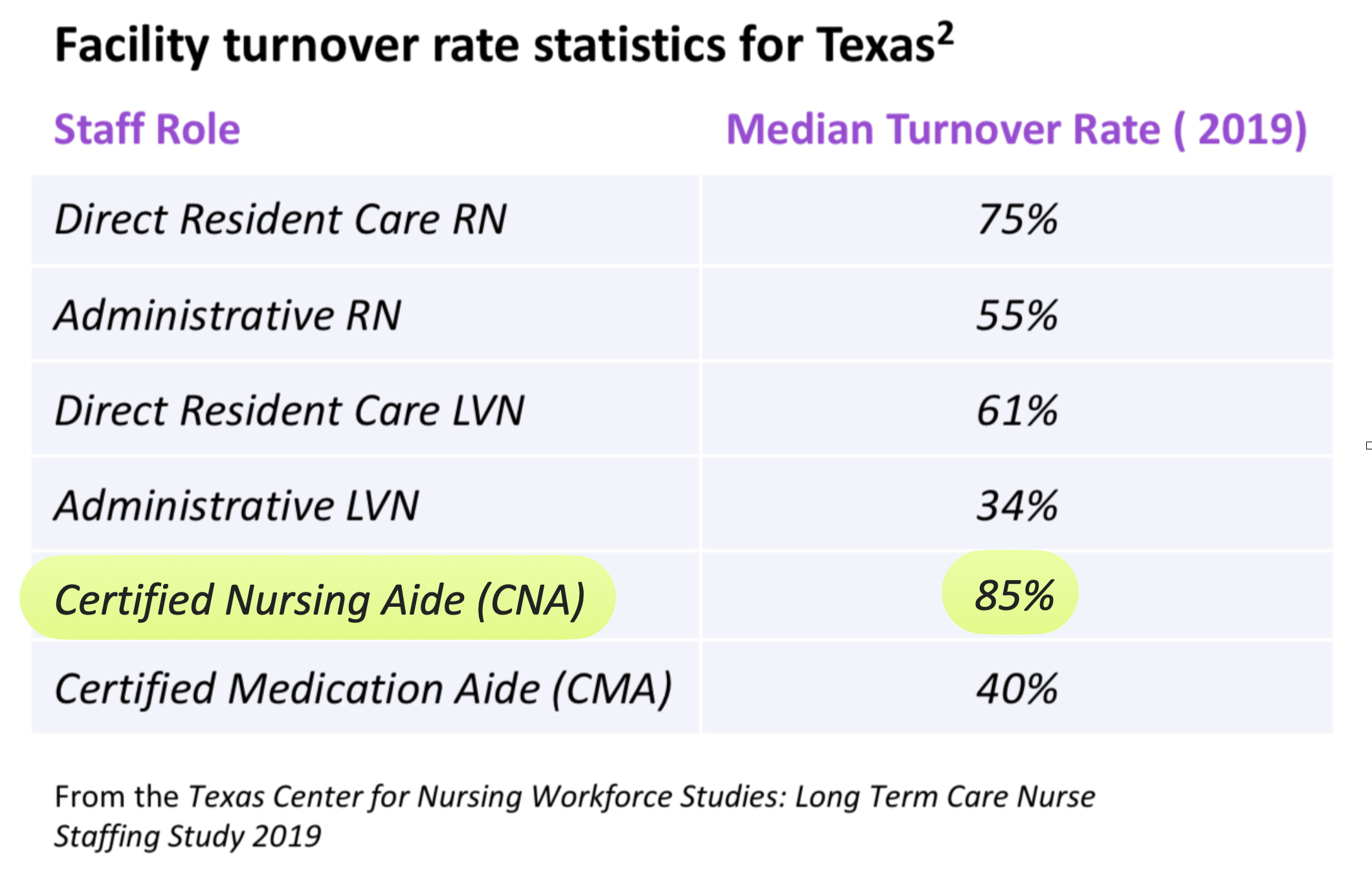
The data confirmed the scale of the problem. Median annual turnover for Certified Nursing Aides in Texas was 85%, with many facilities exceeding 100% per year — a cycle that made institutional knowledge, and therefore infection control, impossible to sustain.
This reframed the problem entirely. Protocols weren't failing because of bad design — they were failing because of a broken relationship between staff and their workplace. That had to be addressed first.
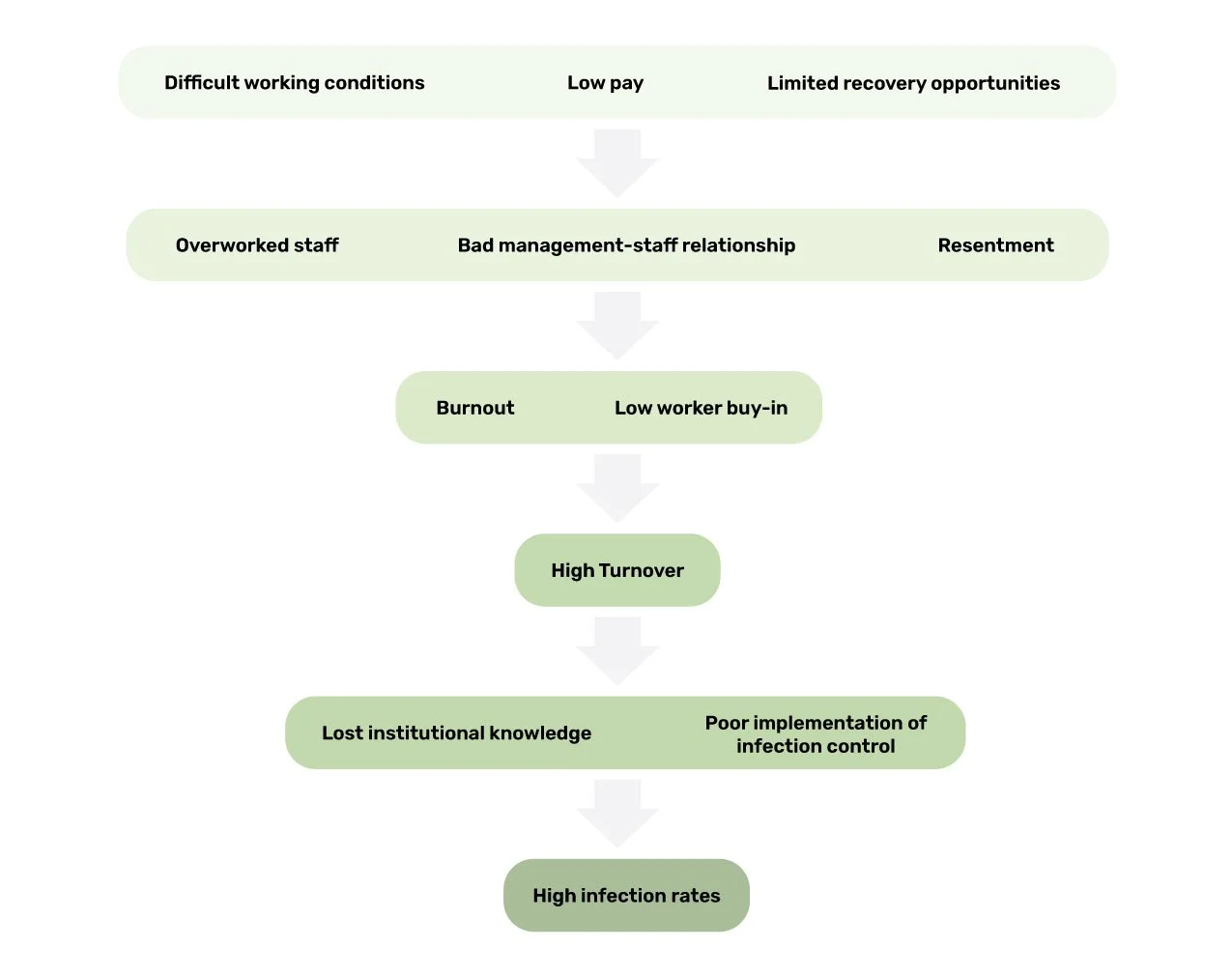
Causal flow diagram | Depicts underlying forces at play
Second Pilot - Targeting Latent Workforce Conditions
The design brief
Two guiding questions shaped our approach: How might we help staff feel valued and supported? How might we help staff recharge throughout their shift?
Primary research revealed that most facilities lacked any dedicated space for staff to rest and recover between shifts — a gap that compounded existing dissatisfaction and accelerated attrition. During COVID-19, when occupational stress reached unprecedented levels, the absence of these spaces became critical.
The solution - Decompression zones
The intervention was clear: create a dedicated staff recovery space inside facilities where none existed. The solution had to work within minimal budgets, adapt to highly variable floor plans, and be simple enough for volunteer organizations to implement independently. And given the intensity of the work environment, the space had to maximize psychological recovery in the shortest possible time.
This led to the development of a scalable, custom-designed decompression zone framework — deployable across regulated care facilities without dedicated design staff or significant capital investment.

A multi-sensory experience
Our solution was inspired by the Recharge Rooms built for Mount Sinai Hospital in New York City. Like those spaces, we leveraged calming sensory experiences to create a maximally relaxing environment. Components used to create a relaxing space included: warm lighting, elements from nature like plants and natural imagery, essential oils diffusers, and non-clinical materials.

The break space before our redesign.
Facility A
A multi-use break space
The break space at Facility A needed to serve multiple functions. The room contained the locker area, time card station and lunch table. For our transformation we set the budget at $300 and opted to use existing furniture onsite.
Concept Images

A Cost-Effective Model
In order for this redesign to be replicable by other facilities, we restricted ourself to a very low budget. In order to achieve the relaxing environment we envisioned, we focused on improving the sensory elements of the space. We added a projector that showed videos of natural landscapes accompanied by the soft sound of that environment. We also lowered the lighting and increased its warmth.

A breakdown of our expenses.


Final Design
With only $300 we were able to transform this cramped, clinical space into a welcoming, comfortable area for staff to relax.
“As soon as you enter you have a peace that comes over you.”
The break space after our redesign.


Our solution is cost-effective, adaptable to a variety of spaces and easy to install with limited design experience.
Facility B
An unused “spa” room

The “spa” room before our redesign.
Facility B was in many ways a more challenging space. Although we did not need to accommodate other uses of the space as a lunchroom, etc. our design needed to accommodate an out-of-use toilet and bathtub. These two items were not in use, but could not be removed from the space. We decided to use inexpensive foam panels and bamboo fencing to conceal the objects. Our budget for this space was $400 and we were able to introduce more textural items, like rugs and pillows to make the space more cozy. We used two chairs the facility had onsite and purchased two additional stools to increase seating capacity.
Before

After

Design Phase


Sketchup models

Final Design
Our final design utilized many of the same elements as Facility A. We created cozy lighting with battery-powered candles, lanterns and string lights. We introduced natural imagery with the projector and several artificial plants. We also included an essential oils diffuser and softer materials.
The break space after our redesign.
“Staff feedback has been nothing but praise.”
-
![]()
The unused toilet is now concealed with bamboo fencing, adding more natural materials to the space.
-
![]()
The bamboo screen covers the unused bathtub and provides a backrest for the two stools.
-
![]()
We repurposed two armchairs from the facility for more comfortable seating.
-
![]()
Pillows add texture and comfort.



